Ischemic Mitral Regurgitation
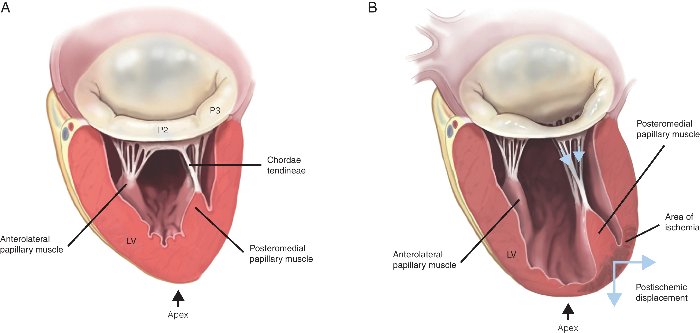
Clinical Problem: Ischemic mitral regurgitation (IMR) is leakage of the mitral valve in patients surviving a heart attack or chronic coronary artery disease. In these patients the injured and dilated ventricle tethers on the mitral valve and restricts its proper closure, causing a gap between the leaflets in systole. Due to the high trans-mitral gradient across the mitral valve, a large amount of blood can regurgitate through this small gap, increase left atrial pressure and changes in pulmonary hemodynamics. Our laboratory is interested in defining the mechanisms causing IMR in humans, develop new techniques to repair IMR.
|
IMR Mechanism: Traditional understanding of IMR teaches us that ischemic injury to the LV causes left ventricular dilatation, which tethers the mitral valve leaflets and restricts their proper closure. While this is accepted by most clinicians, in the real clinical world several patients with small ventricles present with severe IMR, while those with large ventricles do not have any IMR. We are investigating the mechanisms underlying this divergence from accepted dogma in two ways - (Goal 1) Use cardiac MRI in patients to identify localized myocardial mechanics that perturb the mitral valve force balance, and confirm those in animal models; and (Goal 2) Investigate if mitral valve leaflets in some patients become fibrotic and less compliant/mobile due to increased circulating inflammatory markers after an infarction; and if these patients are more prone to develop IMR irrespective of their LV size.
|

|
|
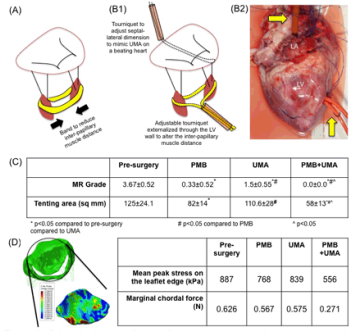
New Techniques to Repair IMR: Traditional surgical repair of IMR focuses on implanting an undersizing ring annuloplasty onto the mitral annulus to reduce its size and close the gap between the leaflets in systole. This technique works for the short term, but recurrent IMR within 1 year is a significant problem in these patients. Our group is investigating a technique based on our observations in human patients to repair IMR - papillary muscle approximation. We found in humans with IMR that loss of lateral shortening of the distance between the two papillary muscles has a strong correlation with severity of IMR. We thus hypothesized that approximating the papillary muscles might improve mitral valve force balance and ensure better coaptation. In appropriate models of IMR, we are investigating the impact of this technique on restoring mitral valve coaptation and long term durability.
|
|